By Connor Hulme, SPT
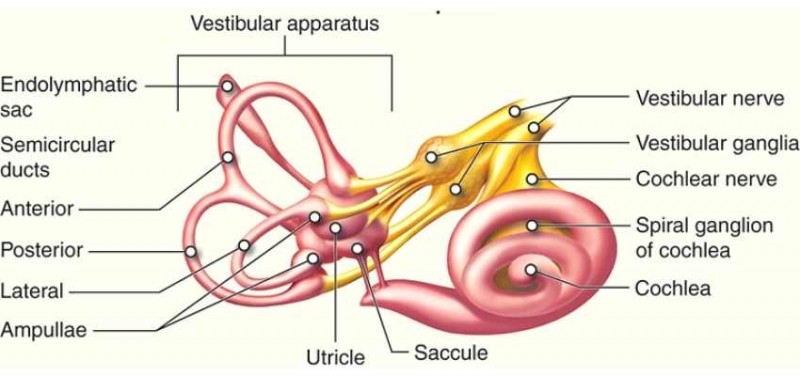
Structures of the Vestibular Apparatus. This work by Cenveo is licensed under a Creative Commons Attribution 3.0 United States (http://creativecommons.org/licenses/by/3.0/us/).
About BPPV
This type of vertigo is the most common type of vestibular disorder, which occurs when otoconia are dislodged from otolith organs. The two types of BPPV are known as canalithiasis and cupulothiasis. To distinguish one type over the other, the therapist completes a testing procedure known as the Dix-Hallpike maneuver. Alternative tests include the side-lying test which, like Dix-Hallpike examines the posterior or anterior canal. If the therapist suspects involvement of the horizontal canal, the Roll test will be used as the assessment procedure.
- Canaithiasis is present when vertigo symptoms last 30-90 seconds after testing, followed by fatigue. This theory states that otoconia are dislodged from the utricle and saccule and are free floating in the semicircular canal.
- Cupulothiasis is present when vertigo symptoms last more than 90 seconds after testing, which is not followed by fatigue. This theory states that otoconia are adhered to the cupula.
Positional vertigo is another vestibular disorder which can easily be confused with BPPV. This type of vertigo only occurs with positional head movements such as looking up, down, and/or with transitional movements such as rolling in bed.
Considerations
Prior to testing for involvement of the anterior or posterior canals, the therapist should first examine for Vertebrobasilar Insufficiency (VBI). This examination procedure occludes blood flow to the brain and is repeated on both sides. Testing is positive when the patient has nausea, visual disturbances, and or syncope.
After being treated for BPPV patients should avoid fast head movements up, down, and side to side for the remainder of the day. To decrease the chance of re-dislodging otoconia after treatment, patients should keep the head in a neutral position for the remained of the day.
Precautions for BPPV Examination
- Cervical stenosis
- Limited cervical ROM
- Down syndrome
- Cervical radiculopathy
- Paget’s disease
- Ankylosing spondylitis
- Low back dysfunction
- Spinal cord injuries
- Morbid obesity
- Vertebrobasilar insufficiency (+)
BPPV Treatment
Canalith Repositioning Maneuver (AKA Epley’s Maneuver)
- This procedure is used when treating either the anterior or posterior canals. The goal of this treatment is to get the free floating otoconia to return to the utricle and saccule.
Liberatory Semont Maneuver
- This procedure is used to treat patients with BPPV symptoms consistent with cupulothiasis. The goal of this treatment is to get the otoconia to dislodge from the cupula and return to the utricle and saccule.
*Patients are likely to experience nystagmus with positional changes during both treatment procedures.
Terminology
- Otoconia: calcium carbonate crystals housed within the otolith organs
- Otolith organs: utricle & saccule
- Utricle – part of the peripheral vestibular system that responds to horizontal, linear movement
- Saccule – part of the peripheral vestibular system that responds to vertical, linear movement
- Both the utricle and saccule contain otoconia
- Cupula: hair cells that sense head motion
- Syncope: à sudden loss of consciousness
Benign Paroxysmal Positional Vertigo (BPPV) is just one of the conditions that Capital Area Physical Therapy & Wellness therapists treat. (See a BPPV patient review). If you live in the Capital Region, we have a clinic near you. For additional information, contact us at 518-289-5242 to make an appointment.